

Medical students and residents are infrequently taught and we are often asked about basic coding skills.
Today we will review basic outpatient/office E/M coding after the 2021 updates. Come back next week for sample cases to help understand. As always, please consult with your medical billers/coders should you have questions.
If you are looking for a reliable billing partner, National Revenue Consulting offers full-service medical billing and coding. Please contact us today to schedule a time. Please share this blog post with others who may need education. Should your office or team need medical billing/coding education, please do not hesitate to reach out.
E/M Codes are determined by one of two options:
- Medical Decision Making
- Number/complexity of problems addressed
- Amount/complexity of data reviewed
- Risk of complications and/or morbidity or mortality of patient management
- Total Provider Time on the Date of Service (DOS)
Prior to 2021, history and examination were key elements of code selection. That is no longer the case. History and examination of the patient should still be done as medically appropriate and documented.
We will talk about each of these in detail and then next week will show some examples!
Medical Decision Making
Medically appropriate history and/or exam must be documented
To support a given code level, 2 out of 3 elements of MDM for that code level must be met or exceeded
1. Number and complexity of problems addressed
• A problem is addressed or managed when it is evaluated or treated at the encounter by the physician or APP reporting the service
• Referral without evaluation (by history, exam, or diagnostic study) or consideration of treatment does not qualify as being addressed
2. Amount and/or complexity of data to be reviewed and analyzed
• Tests, documents, orders, or independent historian(s) – each unique test (as identified by a CPT code), order, or document is counted to meet a threshold number
• Independent interpretation of tests
• Discussion of management or test interpretation with external physician/APP/or appropriate source
3. Risk of complications and/or morbidity or mortality of patient management
• Includes possible management options selected and those considered, but not selected, after shared medical decision making with the patient and/or family
The four levels of MDM will be maintained from prior years:
- Straightforward (2)
- Low (3)
- Moderate (4)
- High (5)
Time Requirements:
- Time may alternatively be used to select a code level for office/outpatient services
- Time may only be used for selecting the level of the other E/M services when counseling and/or coordination of care dominates the service
- Time will be shown below in the E/M Coding Tool
E/M Coding Tool
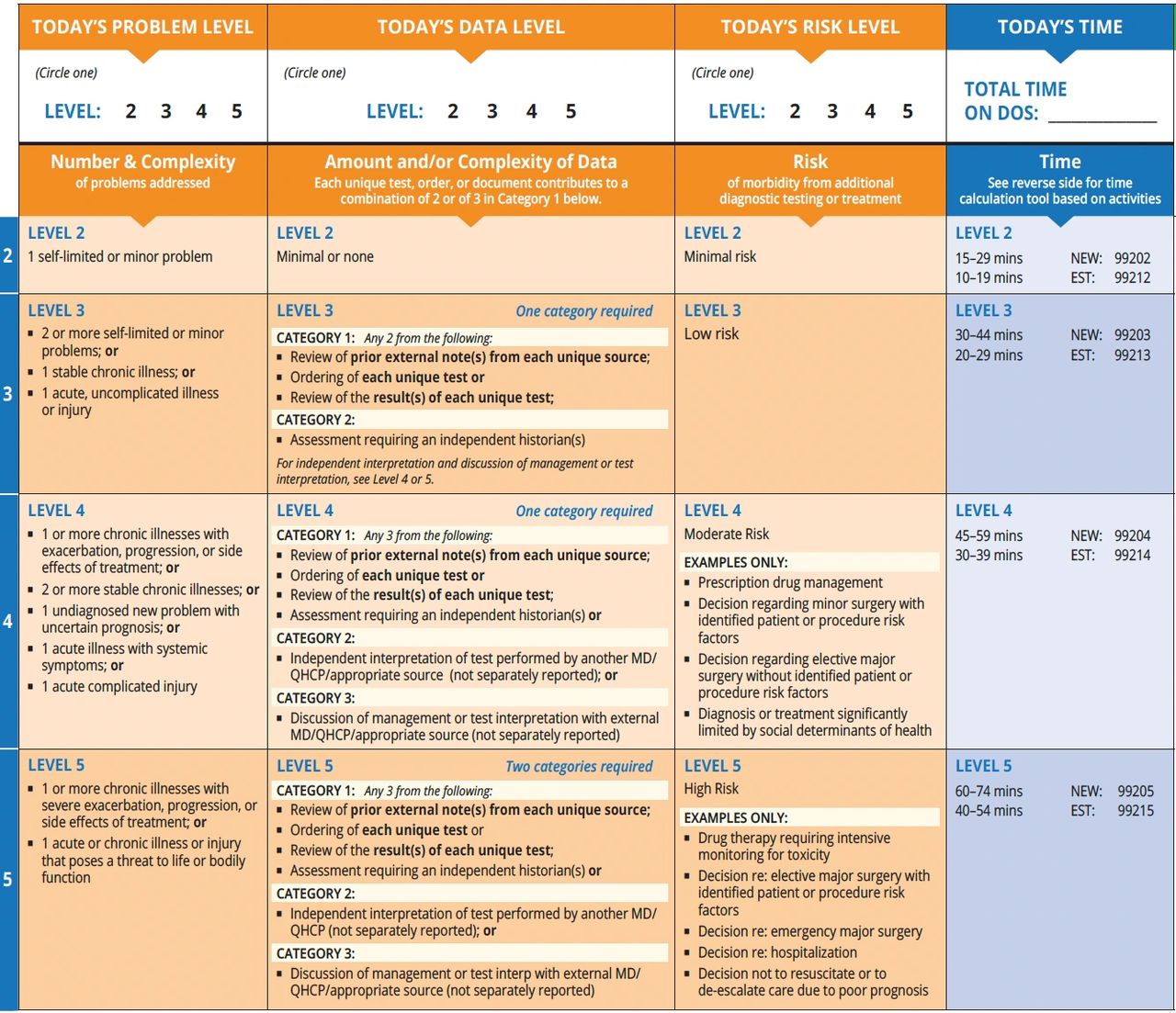
*Pediatric EHR Solutions Resource for E/M Coding
Self-limited or minor problem
- Runs a definite and prescribed course, is transient in nature, and is not likely to permanently alter health status
Stable, chronic illness
- Expected duration of at least a year or until the death of the patient
- “Stable” is defined by the specific treatment goals for an individual patient; a patient that is not at their treatment goal is not stable, even if the condition has not changed
Acute, uncomplicated illness or injury
- Recent or new short-term problem with low risk of morbidity for which treatment is considered
- Little/no risk of mortality with treatment and full recovery without functional impairment is expected
- The problem that is normally self-limited or minor, but is not resolving consistent with a definite and prescribed course
- Examples may include cystitis, allergic rhinitis, or a simple sprain
Chronic illness with exacerbation, progression, or side effects of treatment
- Chronic illness that is acutely worsening, poorly controlled, or progressing with an intent to control the progression and requires additional supportive care or requiring attention to treatment for side effects
- Does not require consideration of the hospital level of care
Undiagnosed new problem with an uncertain prognosis
- A problem in the differential diagnosis that represents a condition likely to result in a high risk of morbidity without treatment
- An example may be a lump in the breast
Acute illness with systemic symptoms
- Illness that causes systemic symptoms and has a high risk of morbidity without treatment
- For systemic general symptoms (fever, body aches, or fatigue) in a minor illness that may be treated to alleviate symptoms, shorten the course of illness, or to prevent complications, see the definitions for “self-limited or minor” or “acute, uncomplicated.”
- Examples may include pyelonephritis, pneumonitis, or colitis
Independent interpretation
- Interpretation of a test for which there is a CPT code and an interpretation or report is customary
- Does not apply when the physician or APP is reporting the service or has previously reported the service for the patient
- A form of interpretation should be documented but need not conform to the usual standards of a complete report for the test
Appropriate source
- Includes professionals who are not health care professionals, but may be involved in the management of the patient
- Examples include lawyers, parole officers, case managers, teacher
- Does not include discussion with family or informal caregivers


